The Adrenal Blueprint: Pregnenolone Steal & The HPA Collapse
The Medical Matrix diagnoses burnout as a psychological condition — a weakness of mind requiring rest, therapy, and antidepressants. Sovereign bio-physics reveals the physical architecture of what is actually failing: a master precursor hormone being systematically stolen in real-time, a feedback loop that has lost its calibration point, and a cascade of hormone depletions that standard blood panels are structurally designed to miss. Burnout is not a mindset problem. It is a terrain problem with a precise biological address.
The Vessel does not simply "burn out."
It executes a logical sequence of triage decisions under sustained energetic threat — and each decision depletes the next system downstream. The adrenal glands are not malfunctioning. They are fulfilling their survival mandate at the cost of every other hormonal system in the body. When we understand the sequence, we can interrupt it — not with suppression, but with precision restoration.
The adrenal collapse operates across four distinct bio-physical stages. Each stage has a different mechanism, a different terrain signature, and a different sovereign intervention point.
Pillar I: The Cortisol Architecture — Why Cortisol Is Not Your Enemy
The HPA axis, the daily voltage rhythm, the intelligent alarm system.
The Mechanism
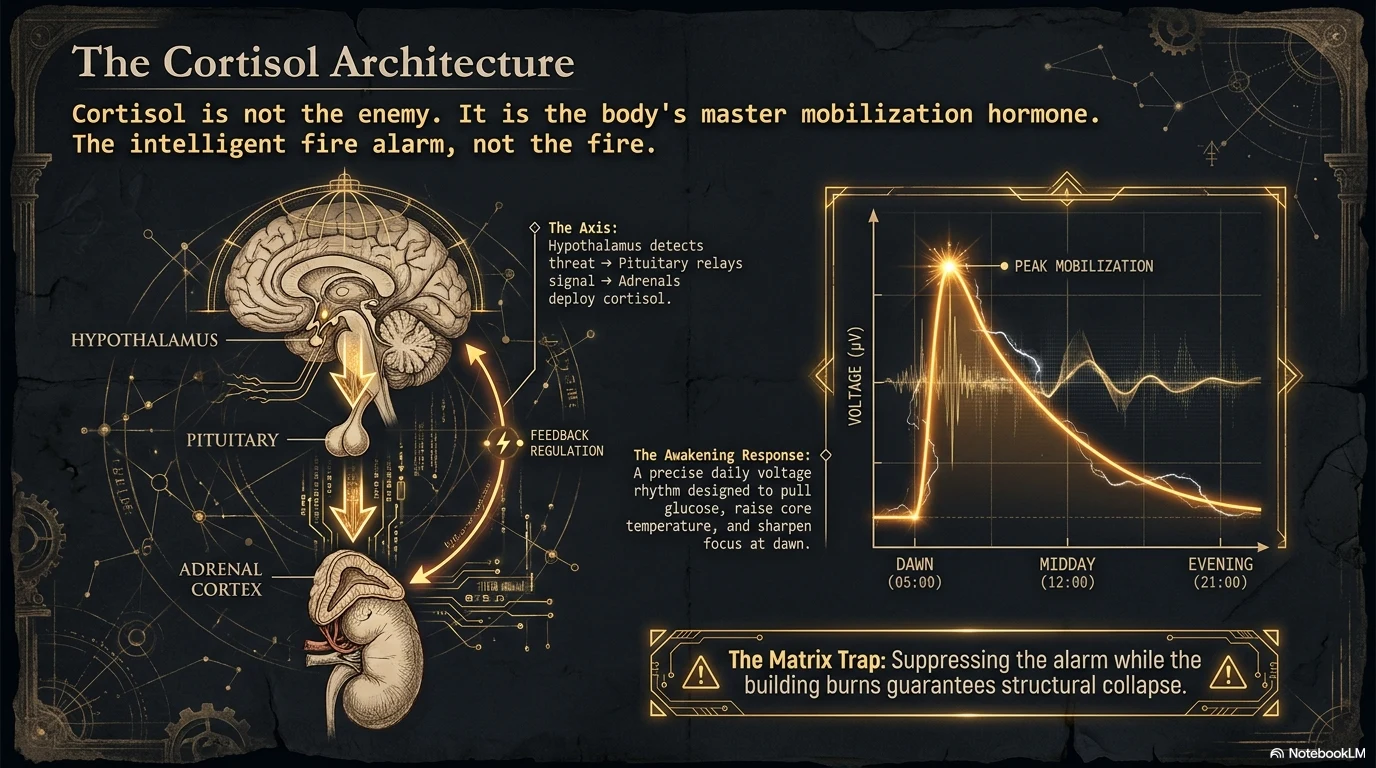
Cortisol is not stress. Cortisol is the body's master mobilisation hormone — a precision instrument that evolved over millions of years to save your life in the face of genuine threat. At dawn, cortisol spikes to pull glucose from storage, raise core temperature, sharpen focus, and prepare the cardiovascular system for the demands of the day. This is the Cortisol Awakening Response — a tightly calibrated voltage signature that should peak within 30 minutes of waking and decline steadily across the afternoon toward evening rest.
The architecture is elegant: the hypothalamus detects a stressor and releases corticotropin-releasing hormone (CRH). The pituitary responds with adrenocorticotropic hormone (ACTH). The adrenal cortex converts that signal into cortisol. Cortisol then loops back to the hypothalamus and pituitary to signal: enough — stand down. This negative feedback loop is the self-correcting intelligence of the HPA axis.
The Matrix Trap: The pharmaceutical model treats elevated cortisol as the problem and pursues suppression. But cortisol is the fire alarm, not the fire. Suppressing the alarm while the building burns guarantees collapse. The terrain model asks: why is the alarm still active? What is the sustained threat the system cannot resolve?
The Sovereign Protocol: Restore the Rhythm
Before any botanical intervention, the daily cortisol architecture must be re-established. Light exposure within 10 minutes of waking activates the suprachiasmatic nucleus and anchors the Cortisol Awakening Response. Darkness after sunset allows melatonin to rise and cortisol to fall. These are not lifestyle suggestions — they are bio-electric switches that govern the entire HPA feedback loop.
Pillar I Protocol — Anchor the Architecture
Morning: Activate the Axis- Direct sunlight within 10 minutes of waking — retinal photoreceptors signal the hypothalamus to initiate the Cortisol Awakening Response on schedule. This single habit recalibrates the entire daily cortisol curve.
- Eleuthero (Eleutherococcus senticosus), 300–600mg: Siberian adaptogen that supports morning adrenal output without overstimulating the axis. Taken at wake-up, it anchors the morning peak without creating the afternoon spike that disrupts the rhythm. Source Eleuthero →
- No artificial blue light after sunset — screens, overhead lighting, and phones emit the same spectral frequency as midday sun. The hypothalamus reads this as ongoing threat and delays the cortisol descent. The adrenals stay active. Sleep fails to restore the terrain.
- Ashwagandha KSM-66 (300–600mg): Evening administration recalibrates the HPA axis toward parasympathetic dominance. GABA-A receptor activation reduces limbic over-activation — the brain stops signalling emergency at midnight. Source Ashwagandha →
Pillar II: Pregnenolone Steal — The Hidden Architecture of Burnout
The master precursor, the hormonal triage decision, the collapse no blood test catches.
The Mechanism
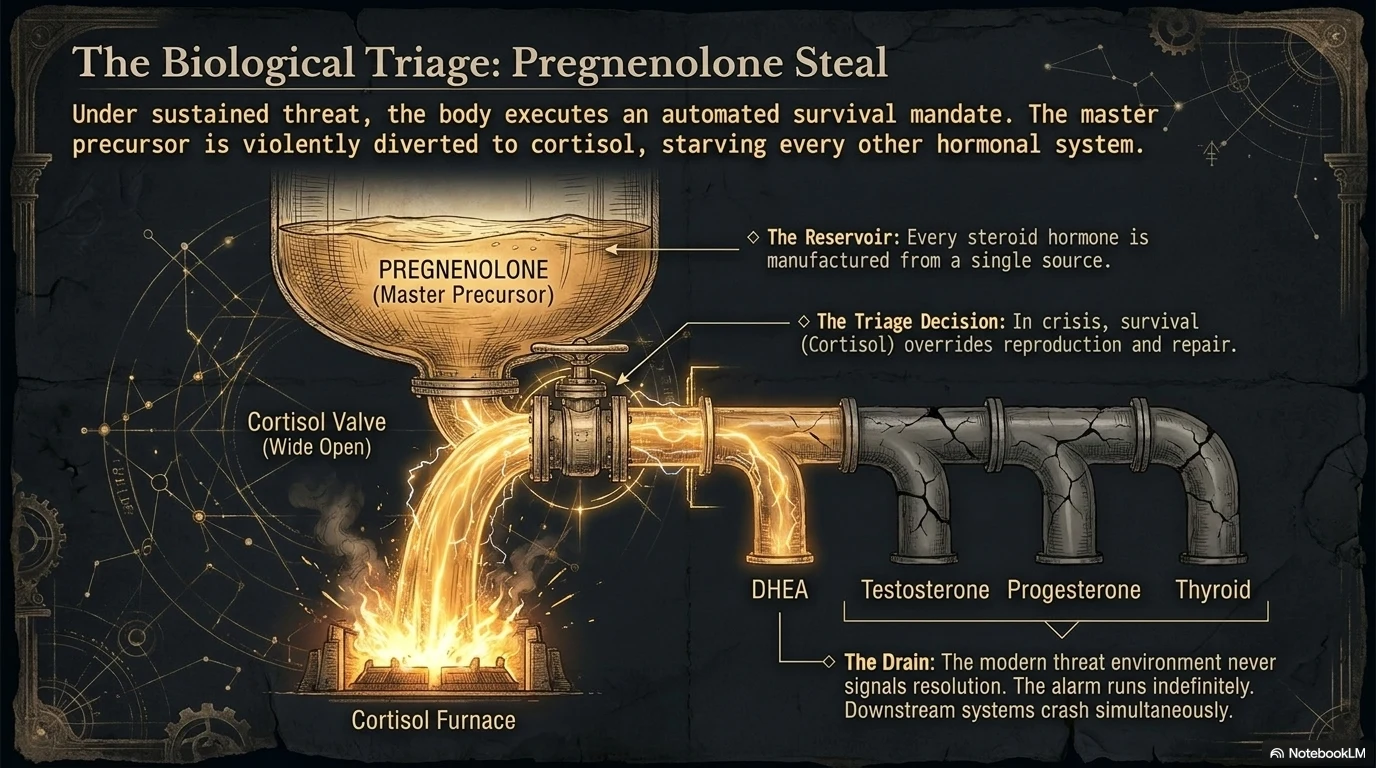
Every steroid hormone in the human body — cortisol, DHEA, testosterone, progesterone, oestrogen, aldosterone — is manufactured from a single master precursor: pregnenolone. Under conditions of sustained stress, the body executes an automated triage decision: redirect pregnenolone toward cortisol production first, at the expense of every other downstream hormone.
This is pregnenolone steal. It is not a pathology. It is survival logic. In a genuine crisis, cortisol matters more than testosterone, progesterone, or DHEA. The problem is that the modern threat environment never signals resolution. Chronic workplace pressure, financial anxiety, inflammatory food, and artificial light after sunset keep the alarm permanently active. The triage decision runs indefinitely. All downstream hormones fall — simultaneously — over months and years.
The clinical picture: fatigue, low libido, mood instability, poor recovery, and cold intolerance — presenting across all ages and genders. Standard blood panels measure cortisol (often still within range in the morning), check TSH, and find nothing actionable. The pregnenolone drain is upstream of every measurement they take.
The critical insight: You cannot supplement DHEA, testosterone, or progesterone back into normal range while the pregnenolone drain is active. The downstream deficits are a symptom of the upstream triage. Fill the reservoir — stop the steal — and the downstream hormones begin to recover on their own architecture.
The Sovereign Protocol: Stop the Drain
Pillar II Protocol — Interrupt the Steal
Reduce the Cortisol Demand- Rhodiola rosea (200–400mg standardised extract, morning): Adaptogen that operates directly at the adrenal level — modulates the cortisol release signal without suppressing it. Active compounds salidroside and rosavins inhibit MAO-A and MAO-B, elevating the serotonin and dopamine precursor pool, which reduces the panic signalling from the limbic system that drives HPA activation. The adrenals produce less cortisol because the brain is sending fewer distress signals. Source Rhodiola →
- Phosphatidylserine (100–300mg): Phospholipid that directly blunts the ACTH signal from the pituitary — the precursor to cortisol release. Reduces exercise-induced cortisol spikes and post-stress cortisol persistence. Source Phosphatidylserine →
- Licorice Root (Glycyrrhiza glabra, 400–600mg standardised to glycyrrhizin): Inhibits 11β-hydroxysteroid dehydrogenase type 2 — the enzyme that breaks down cortisol. By extending the half-life of circulating cortisol, the adrenals are called upon less frequently to produce more. This reduces total adrenal burden without suppressing the axis. Note: not indicated in hypertension — glycyrrhizin elevates aldosterone. Use deglycyrrhizinated licorice (DGL) if blood pressure is a factor. Source Licorice Root →
Pillar III: The Downstream Collapse — What Falls When Cortisol Wins
DHEA, testosterone, thyroid conversion, and the hippocampal cost.
The Mechanism
Once the pregnenolone drain is sustained beyond several months, four downstream systems collapse in sequence. Understanding the sequence matters — because treating any one of them in isolation produces partial and temporary results.
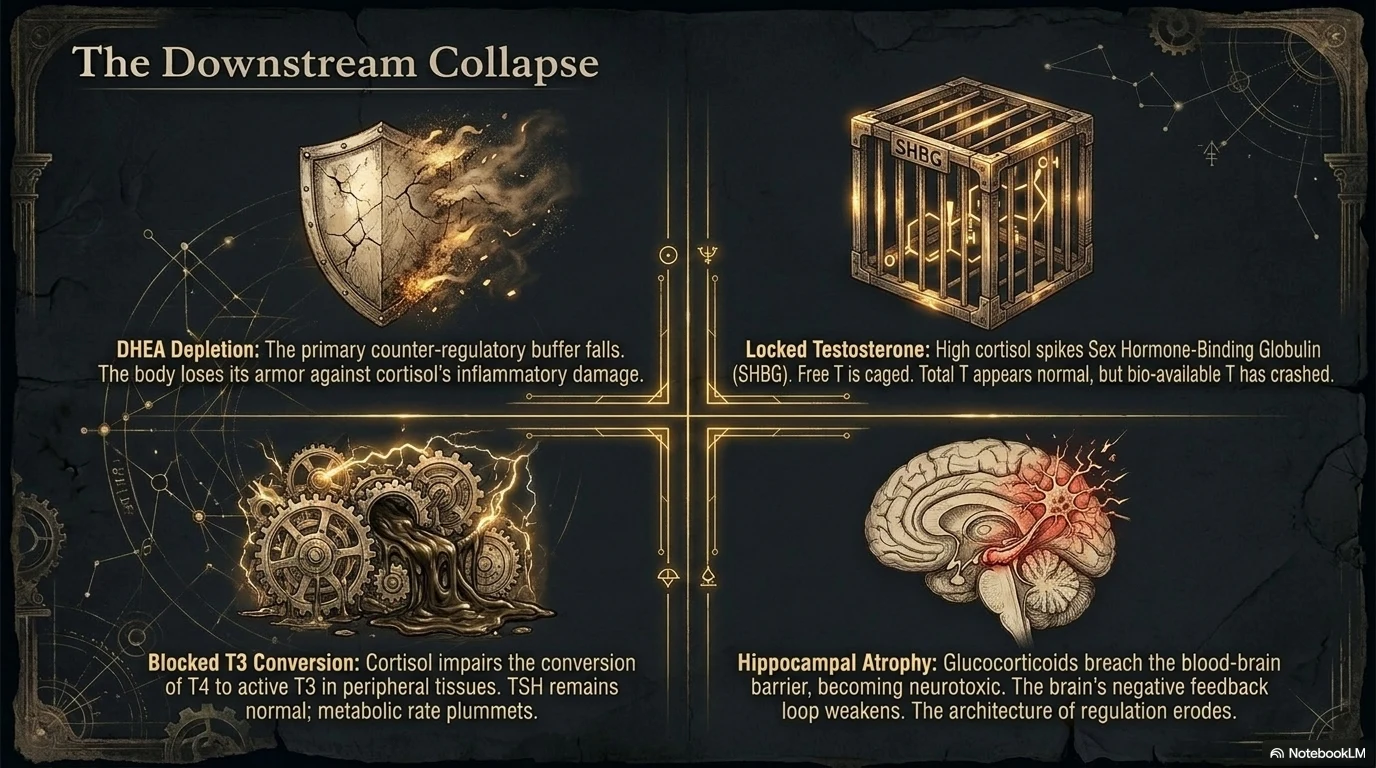
DHEA: The first hormone diverted from. DHEA is the direct precursor to testosterone and oestrogen, and functions as a counter-regulatory hormone to cortisol — in healthy terrain, the two rise and fall in opposition. In pregnenolone steal, DHEA falls as cortisol rises. As DHEA depletes, the body loses its primary buffer against the inflammatory damage cortisol causes at high sustained levels.
Testosterone: Falls downstream of DHEA depletion. Simultaneously, chronically elevated cortisol raises Sex Hormone-Binding Globulin (SHBG) — which binds free testosterone out of circulation. Total testosterone on a blood panel may appear normal while free, bioavailable testosterone has collapsed. The man who is told his levels are "fine" and still cannot recover, sleep, or build muscle is almost always in this state.
Thyroid conversion: Elevated cortisol impairs the conversion of T4 (inactive) to T3 (active) in peripheral tissues. TSH remains normal. T4 remains normal. The T3 that actually enters the cell and drives metabolic rate is insufficient. Cold hands, hair loss, low resting heart rate, and morning brain fog are the signature. Doctors see normal TSH and conclude the thyroid is functioning. The conversion failure is invisible to the standard panel.
Hippocampal atrophy: Chronically elevated glucocorticoids cross the blood-brain barrier and are directly neurotoxic to hippocampal neurons. Hippocampal volume measurably decreases under sustained cortisol exposure — documented across multiple peer-reviewed studies including PMC3230706. The hippocampus houses the primary cortisol receptor density that should signal the hypothalamus to stop the HPA cascade. As it atrophies, the negative feedback loop weakens. Cortisol continues to rise. The architecture of regulation erodes.
The Matrix Trap: Each of these downstream effects generates a separate diagnosis — low testosterone (TRT offered), hypothyroidism (synthetic T4 offered), depression (SSRIs offered), cognitive decline (accepted as aging). Four diagnoses, four prescriptions, zero attention to the upstream pregnenolone drain that is driving all of them from a single address.
The Sovereign Protocol: Restore the Downstream Architecture
Pillar III Protocol — Downstream Restoration
Free the Testosterone- Nettle Root (Urtica dioica root, 300–500mg): Binds Sex Hormone-Binding Globulin directly — reducing the SHBG available to sequester testosterone. As SHBG falls, free testosterone rises from the existing total pool without requiring hormonal supplementation. The testosterone was there — it was simply locked. Source Nettle Root →
- Pine Pollen (tincture, sublingual): Contains plant-source androgens (androstenedione, testosterone, DHEA) delivered sublingually — bypassing first-pass liver metabolism. Acts as a transitional androgen support while the upstream pregnenolone pool recovers. Source Pine Pollen →
- Ashwagandha (300–600mg): Documented to increase T3 and T4 levels in subclinical hypothyroid cases — likely via reduction of the cortisol that was impairing peripheral conversion. As HPA tone normalises, thyroid conversion resumes. Source Ashwagandha →
- Selenium (200mcg, selenomethionine form): Co-factor for the deiodinase enzyme that converts T4 to T3. Without adequate selenium, peripheral conversion stalls regardless of thyroid gland function. Source Selenium →
- Lion's Mane (Hericium erinaceus, dual extract, 500–1000mg): Stimulates nerve growth factor (NGF) synthesis — directly supporting hippocampal neurogenesis. As the terrain's cortisol burden falls, Lion's Mane provides the growth signal that rebuilds what chronic stress degraded. Source Lion's Mane →
- Bacopa monnieri (300mg standardised to 45% bacosides): Adaptogen with documented cortisol-lowering activity and direct hippocampal neuroprotection. Improves memory encoding and recall in cortisol-damaged terrain. 8–12 week minimum protocol required. Source Bacopa →
Pillar IV: The Full Restoration Stack — Rebuilding the Substrate
The sequence, the timing, the three-phase protocol.
The Mechanism
Adrenal restoration cannot be executed as a single botanical intervention. The axis was depleted in sequence — it must be rebuilt in sequence. Attempting to stimulate downstream hormone production before reducing the upstream cortisol demand is like pouring water into a bucket with a hole in the bottom. The order of operations is the protocol.
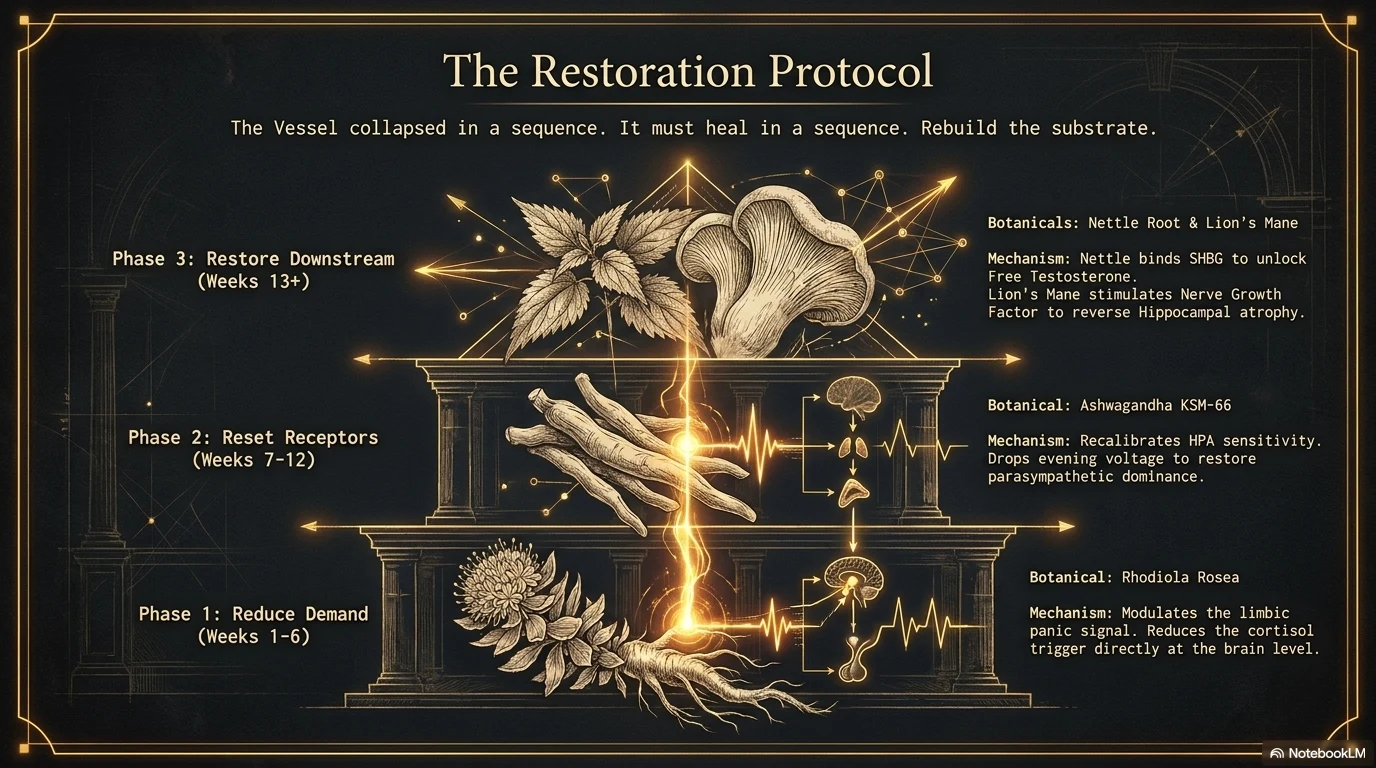
Phase one reduces the cortisol demand and extends cortisol efficiency. Phase two rebuilds the receptor sensitivity of the HPA feedback loop. Phase three restores the downstream hormonal architecture from the now-stable foundation. Each phase requires a minimum of four to six weeks before the next begins.
The Sovereign Protocol: The Three-Phase Restoration
Pillar IV Protocol — The Adrenal Blueprint
Phase 1 (Weeks 1–6): Reduce the Demand- Rhodiola rosea 200–400mg at wake-up — reduces the cortisol trigger signal from the limbic system
- Eleuthero 300–600mg at wake-up — supports adrenal output without overstimulation
- Licorice Root 400–600mg midday — extends cortisol half-life, reduces total adrenal calls
- Remove dietary inflammatory load: seed oils, refined sugar, glyphosate-contaminated grains. The terrain cannot heal under sustained chemical threat.
- Ashwagandha KSM-66 300–600mg evening — recalibrates HPA receptor sensitivity, documented 23% cortisol reduction at 60 days (PMC6979308)
- Reishi mushroom (dual extract, 1–2g) — immune terrain restoration while cortisol has been chronically immunosuppressive; rebuilds the NK cell baseline that cortisol degraded. Source Reishi →
- Anchor the circadian architecture: consistent sleep and wake times, morning light, darkness after sunset. Circadian consistency is the most powerful HPA reset available without a prescription.
- Nettle Root 300–500mg — free the testosterone that SHBG has sequestered
- Pine Pollen tincture — sublingual transitional androgen support
- Lion's Mane 500–1000mg — hippocampal NGF stimulation and neurogenesis
- Selenium 200mcg selenomethionine — restore T4→T3 conversion capacity
- At this stage, if the Phase 1 and 2 protocol has held, morning cortisol rhythm should be re-established and downstream hormones will recover toward baseline without external hormonal supplementation.
Conclusion: The Architecture Always Had an Address
The burnout epidemic is not a modern mystery. It is a predictable architectural collapse in a terrain that has been under sustained, unresolved threat — from chronic psychological pressure, industrial food, artificial light, and the absence of biological recovery rituals that our physiology requires to reset the HPA axis.
The Medical Matrix treats the downstream wreckage as a collection of separate diseases. Sovereign bio-physics traces every symptom back to a single upstream mechanism — the pregnenolone steal — and addresses it at the source. The adrenal glands did not fail. They succeeded at their survival mandate so completely, for so long, that they depleted the reserves of every other system in the body.
The Sovereign summary:
Stop treating burnout as a psychological failure. Locate the mechanism. Interrupt the steal. Rebuild the substrate in sequence — not all at once, not with suppression, but with precision restoration aligned to the body's own repair architecture.
The Vessel collapsed in a sequence. It heals in a sequence. Give it the right tools in the right order, and the architecture rebuilds itself.